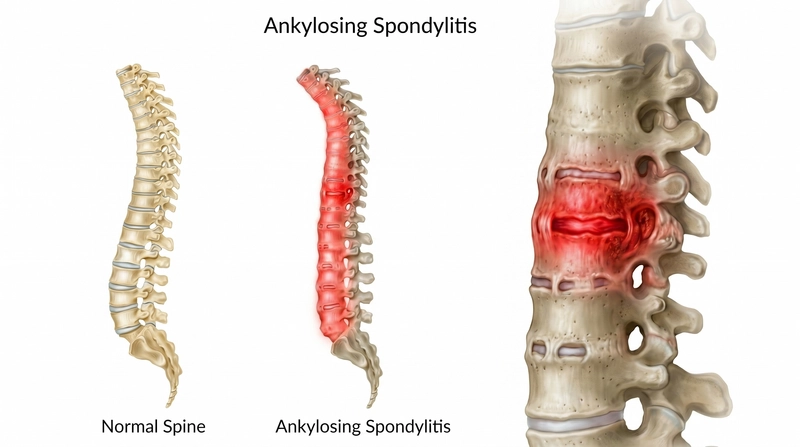
Ankylosing Spondylitis
A chronic, progressive inflammatory disease of the spine that causes pain, stiffness, and reduced mobility — and can lead to permanent fusion of the vertebrae if left unmanaged. Early diagnosis and timely intervention are critical.
Symptoms
Ankylosing Spondylitis (AS) typically begins between ages 17 and 40 with early morning stiffness and back pain. Without proper management, it progresses — gradually restricting movement and, in severe cases, causing the spine to fuse into a fixed, immobile position.
17–40
typical age of onset in early adulthood
Chronic
progressive — worsens without management
HLA-B27
key genetic marker present in ~90% of AS patients
How AS progresses if left untreated:
Early morning stiffnessImproves with movement
Chronic back painSacroiliac joints first
Reduced mobilityLumbar & thoracic spine
Bony bridgingOsteophytes form
Spinal fusion"Bamboo spine" — irreversible
Extra-spinal features:
Eye inflammationUveitis / iritis — pain, redness, blurred vision
Chest tightnessRib joint involvement — restricted breathing
Bowel inflammationAssociated with ulcerative colitis / Crohn's
Spinal symptoms you may experience:
Early morning stiffness and pain in the lower back, neck, and hips — worst on waking, easing with movement
Increasing pain and difficulty with movement — bending, turning, or straightening the spine
Pain radiating from the buttocks into one or both legs — sacroiliac joint involvement
Pain spreading from the neck or upper back into the hands or fingers when discs are involved
Tingling, numbness, burning, or weakness in legs, feet, hands or fingers (disc involvement)
Pain worsening with prolonged rest or sitting — characteristically relieved by activity
Loss of bladder or bowel control in severe cases with cord involvement
Progressive loss of spinal flexibility — difficulty looking over the shoulder or bending forward
Causes
The exact cause is not fully known, but some common contributing factors include:
Genetics (HLA-B27, Anti CCP, ANA, CRP).
Urethritis
Ulcerative colitis
Conjunctivitis
Klebsiella infection
Diagnosis
A detailed history and physical examination are central to diagnosing AS. Characteristic features — early morning stiffness improving with activity, sacroiliac joint tenderness, and reduced spinal mobility — combined with genetic markers and imaging findings confirm the diagnosis. Key imaging findings include loss of lumbar lordosis, bridging osteophytes, and the classic "bamboo spine" on X-ray.
X-ray
MRI
CT scan
DEXA scan
HLA-B27
Sr. IgA / CRP
X-ray reveals loss of lumbar lordosis, sacroiliac joint erosion, bridging osteophytes, and in advanced disease — bamboo spine. MRI detects early inflammation before structural changes appear on X-ray, making it preferred for early diagnosis. HLA-B27 confirms genetic susceptibility. Serum IgA and CRP reflect disease activity and guide treatment decisions.
Treatment
Treatment of AS depends critically on the stage of the disease — specifically whether spinal fusion has occurred. Early-stage AS without fusion responds well to non-surgical treatment. Once fusion is established, surgical options become the primary consideration.
General measures — essential for all patients
Patient education — understanding the nature, progression, and self-management of AS
Family education — awareness of the condition's demands and how to support the patient
Genetic counselling — guidance on hereditary risk for family members
Occupational therapy — adapting daily activities and work to reduce spinal strain
Non-surgical spinal decompression — who is eligible
Patients with early-stage AS who have not yet developed lumbar or cervical fusion, and who also have a concurrent slipped disc, may be eligible for Non-Surgical Spinal Decompression at Spine Science & Beyond.
Early-stage AS — no fusion present at lumbar or cervical spine
Concurrent disc involvement (slip disc / disc bulge) confirmed on MRI
Treatment reduces intradiscal pressure, freeing compressed nerves and relieving pain
Patient is thoroughly counselled on AS progression and long-term outlook
When fusion has occurred — surgical management
In cases where spinal fusion is established, conservative and non-surgical treatments have very minimal to no effect. Surgical intervention becomes the most appropriate and effective option — and the patient is referred and guided accordingly.
Ankylosing Spondylitis is a progressive condition. Early diagnosis and timely treatment are critical to preventing irreversible fusion and preserving long-term spinal mobility.