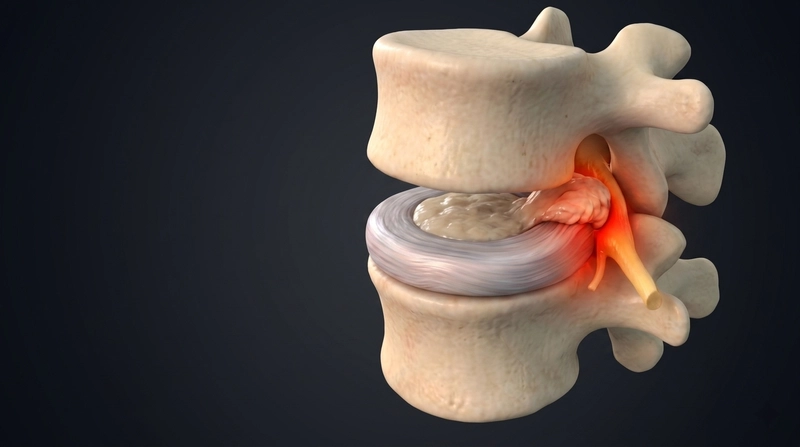
Disc Herniation
Disc herniation is a condition in which the inner soft gel of the disc (nucleus pulposus) slips out from the outer hard layer (annulus fibrosus) and presses on a nerve.
Symptoms
Disc herniation is most common in the lumbar spine (lower back) and second most common in the cervical spine (neck). It represents a more advanced stage than a disc bulge — the inner gel has actually broken through the outer wall, making direct nerve contact more likely and symptoms typically more severe.
L4–L5
most common lumbar level affected
C5–C6
most common cervical level affected
90%
of cases resolve without surgery when treated correctly
Where herniation most commonly occurs:
Most commonLumbar (lower back)L4–L5, L5–S1 — leg pain, foot drop, sciatica
CommonCervical (neck)C5–C6, C6–C7 — arm pain, hand tingling
RareThoracic (mid-back)T8–T12 — chest/abdominal referred pain
Hallmark symptoms of disc herniation:
Sharp, shooting, electric-shock pain radiating down the leg or arm — often described as worse than the back pain itself. This nerve pain is the defining feature that distinguishes disc herniation from simpler back pain.
Foot drop — difficulty lifting the foot when walking, standing, or sitting, caused by compression of the L4–L5 nerve root. This is a red flag requiring urgent assessment.
Other symptoms you may experience:
Increasing pain with lifting and bending, worsening with activity
Morning stiffness that may increase or ease with movement
Pain radiating from the buttocks down one or both legs
Pain worsening with rest, sitting, standing, or walking
Tingling, numbness, burning, or weakness in the legs and feet
Back or neck pain that comes and goes with posture changes
Reduced bladder or bowel control in severe cases
Foot drop or sudden loss of bladder / bowel control are medical emergencies. Seek immediate attention — delayed treatment can lead to permanent nerve damage.
Causes
Disc herniation occurs when accumulated disc damage — from lifestyle, age, or trauma — finally causes the outer ring to tear. In many cases, what feels like a sudden injury is actually the final step in a long degenerative process.
Lifestyle factorsLeading contributor
Sedentary lifestyle reduces the nutrient supply to discs, while poor posture places asymmetric load on the outer ring. Obesity increases compressive forces, and smoking impairs disc blood supply — all accelerating the weakening process.
Sedentary lifestylePoor postureObesitySmokingAlcohol
Occupational strain
Heavy lifting — especially with poor technique — creates sudden high-pressure spikes inside the disc. Prolonged sitting, standing, stooping, or slouching maintain chronic compressive load that gradually weakens the annular fibres.
Heavy liftingProlonged sittingStoopingPoor lifting technique
Sports & sudden impact
Contact sports involving abrupt rotational or compressive forces — football, basketball, rugby, wrestling — can cause acute herniation even in younger patients with otherwise healthy discs.
FootballBasketballContact sportsAbrupt rotational movement
Physical trauma
Road traffic accidents, falls, and direct spinal impact can cause acute herniation — bypassing the usual slow degenerative process — by applying sudden extreme force to a disc.
Road accidentsFallsFractureTumourCyst
Age & degeneration
As discs age, they dehydrate and lose elasticity — making the annulus fibrosus more brittle and prone to tearing under loads that a younger disc would easily withstand.
Degenerative disc diseaseOsteoporosisDisc dehydrationArthritis
Medical & inflammatory conditions
Conditions that alter spinal biomechanics or impair tissue quality increase disc herniation risk significantly — through both mechanical overload and biochemical disc degradation.
ObesityFibromyalgiaScoliosisPregnancyAnkylosing spondylitisSacroiliitis
Diagnosis
A thorough history and physical examination are usually sufficient to diagnose disc herniation and locate the affected level. The doctor will perform a neurological assessment — sensation, reflexes, muscle power, range of motion, and specialised tests — then correlate with imaging.
X-ray
MRI
CT scan
EMG / NCV
DEXA scan
Blood tests
Treatment
Non-surgical spinal decompression
At Spine Science & Beyond, we have successfully treated thousands of patients with disc herniation — without surgery, medications, injections, or exercise programs.
No longer relying on:
Physiotherapy
Surgery
Steroid injections
Painkillers
Exercise alone
Why spinal decompression works:
Targets the root cause — directly reducing the disc herniation compressing the nerve
Completely non-invasive with zero side effects
Creates negative intradiscal pressure, drawing the herniated nucleus pulposus back through the annular tear and freeing the compressed nerve
Improves blood and nutrient circulation to the disc, promoting healing of the annular tear and disc rehydration
Progressively reduces nerve pain, tingling, numbness, and weakness
Improves disc quality and height, reducing the risk of recurrence